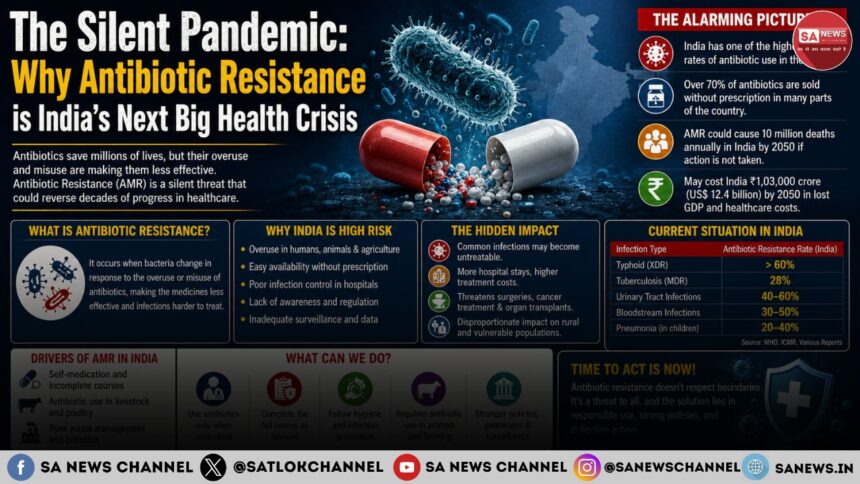
While the world remains on high alert for the next viral outbreak, a far more insidious and quiet health crisis is unfolding right under our noses. Antimicrobial Resistance (AMR), often called the “Silent Pandemic” is rapidly turning common, once-curable bacterial infections into untreatable medical nightmares. Driven by self-medication, over-the-counter misuse of antibiotics, and their widespread use in agriculture, India has emerged as one of the global epicenters of this crisis. If public behavior and regulatory enforcement do not pivot sharply, the foundations of modern healthcare, surgery, and cancer treatments could face catastrophic failure within the coming decades.
- News Highlights on “Silent Pandemic”
- The Mechanics of Selection Pressure
- India’s Unique AMR Landscape
- The Institutional Alarm
- The Roadmap for Containment
- True devotion cures the greatest disease of birth and death
- Core Philosophy on Medicine and Healing
- Prohibited and Recommended Actions
- Charitable Medical Initiatives
- FAQs
- 1. What is the difference between antibiotic resistance and antimicrobial resistance (AMR)?
- 2. Can my body become resistant to antibiotics?
- 3. Why are antibiotics completely useless against the common cold and flu?
- 4. What happens if I stop taking my prescribed antibiotic course early because I feel better?
- 5. How can an ordinary citizen help stop the silent pandemic of AMR?
News Highlights on “Silent Pandemic”
- A Growing Fatal Toll: Drug-resistant bacterial infections are associated with nearly one million deaths annually in India, heavily impacting both neonates and the elderly.
- The Rise of Superbugs: Recent ICMR surveillance has reported carbapenem resistance rates exceeding 80–90% in Acinetobacter baumannii isolates in some hospital settings.
- The Over-the-Counter Catalyst: Unregulated access to Schedule H and H1 drugs allows widespread misuse of antibiotics for viral infections like the common cold, where they offer zero therapeutic benefit.
- The Post-Antibiotic Era Threat: Medical experts warn that without strict intervention, routine procedures like C-sections, joint replacements, and chemotherapy will become life-threatening due to uncontrollable secondary infections.
The Mechanics of Selection Pressure
To understand the gravity of Antimicrobial Resistance, one must look at the microscopic battleground. Bacteria are highly adaptive organisms. When an individual takes an antibiotic, the drug is designed to target specific bacterial mechanisms such as cell wall synthesis or protein translation.
However, if the antibiotic is taken at an inadequate dose, stopped prematurely, or used unnecessarily against a viral infection, it creates a sub-lethal environment. The weaker bacteria die, but the few that possess natural genetic mutations survive. This biological phenomenon, known as selection pressure, allows the resistant strains to multiply rapidly and pass on their survival traits via horizontal gene transfer.
According to ICMR’s ongoing surveillance, common pathogens like Escherichia coli (E. coli) and Klebsiella pneumoniae are showing a steady, year-over-year decline in susceptibility to broad-spectrum antibiotics, pushing clinicians into a corner where they must rely on increasingly toxic or experimental drug regimens.
India’s Unique AMR Landscape
India’s battle with AMR is uniquely complex. The country carries a massive infectious disease caseload, coupled with rapid urbanization and variable sanitation infrastructure. When a resistant strain emerges in an overcrowded urban environment, it spreads far more rapidly through the community and hospital networks than it would in high-income nations.
Furthermore, the cultural habit of “pharmacy shopping” where patients bypass doctors to buy cheap, loose antibiotic capsules directly from local chemists acts as fuel for the fire. Mild respiratory illnesses or episodes of seasonal diarrhoea, which are primarily viral or self-limiting, are routinely treated with powerful fluoroquinolones or third-generation cephalosporins.
The crisis is not restricted to human medicine alone. The livestock and poultry industries widely use antibiotics as growth promoters rather than for treating diagnosed illnesses. These low-dose antimicrobials leach into the soil and groundwater through animal waste, introducing drug residues into our agricultural supply chain and further accelerating environmental resistance.
The Institutional Alarm
The reality inside Indian Intensive Care Units (ICUs) is alarming. The ICMR Antimicrobial Resistance Research and Surveillance Network highlighted that Methicillin-resistant Staphylococcus aureus (MRSA) rates have climbed significantly, now crossing 53%. Even more concerning is the status of Acinetobacter baumannii , a common cause of ventilator-associated pneumonia which leaves doctors with very limited treatment options.
”We are regularly seeing patients walk into community clinics with infections that do not respond to first-line or even second-line oral antibiotics,” says a senior clinical microbiologist based in New Delhi. “When standard empirical therapy fails, a patient who should have been cured in five days ends up spending weeks in an expensive ICU, facing severe financial distress and a much higher risk of mortality.”
The Roadmap for Containment
Mitigating this silent crisis requires an urgent, structural shift across multiple sectors under a unified One Health framework:
- Enforcing Legal Gatekeeping: Strict implementation of the red-line campaign on antibiotic packaging is required. Pharmacies must face severe penalties for dispensing Schedule H and H1 antibiotics without a valid registered medical practitioner’s prescription.
- Institutional Stewardship: Hospitals must implement rigorous Antimicrobial Stewardship Programs (AMSP). Doctors should avoid prescribing broad-spectrum empirical antibiotics before obtaining culture and sensitivity reports, except in life-threatening cases of sepsis.
- Public Education Overhaul: Mass awareness campaigns must teach the public that antibiotics do not cure viral coughs, colds, or flu.
- Investing in Diagnostics: Transitioning from empirical guessing to precise, rapid diagnostic tools will allow doctors to identify the exact pathogen within hours, ensuring targeted narrow-spectrum therapy.
True devotion cures the greatest disease of birth and death
Sant Rampal Ji Maharaj teaches that true spiritual devotion cures the ultimate disease of birth and death. While devotees continue to take medicines and consult doctors, they find that sincere chanting of the true mantras and following the path of the Supreme God Kabir ultimately cures even incurable ailments.
Core Philosophy on Medicine and Healing
Ultimate Cure vs. Temporary Relief: Sant Rampal Ji Maharaj teaches that all physical ailments are the result of past karmas. While doctors and medicines can provide temporary physical relief, only the true worship of the Supreme Almighty can permanently erase the root cause of all suffering.
The Power of Mantras: Devotees share numerous experiences where doctors pronounced diseases incurable, but through the recitation of the mantras and strict adherence to the spiritual rules, they were completely healed.
No Condemnation of Doctors: The philosophy does not forbid taking medicine. Instead, it frames divine intervention as the ultimate remedy when medical science reaches its limits.
Prohibited and Recommended Actions
To attain the grace of the Supreme Lord and see healing, practitioners must strictly follow the code of conduct:
Strictly Prohibited: Consumption of alcohol, meat, tobacco, gambling, and participating in false worship (such as worshipping ghosts, ancestors, or other deities).
Recommended: Receiving Naam Diksha (initiation), consuming charnamrit (holy water), and continuously chanting the true holy names given by the Guru.
Charitable Medical Initiatives
Reflecting the core belief in human welfare, the ashrams associated with Sant Rampal Ji Maharaj regularly organize free medical camps. These camps provide free check-ups, dental treatments, and eye surgeries to the underprivileged, demonstrating a practical blend of community service and spiritual teaching.
To learn more about the complete philosophy, you can read the spiritual literature authored by the Saint Rampal Ji Maharaj, such as Gyan Ganga and Jeene Ki Rah.
FAQs
1. What is the difference between antibiotic resistance and antimicrobial resistance (AMR)?
Antibiotic resistance refers specifically to bacteria becoming resistant to the antibiotics used to treat them. Antimicrobial resistance (AMR) is a broader term that encompasses resistance developed by all types of microbes, including bacteria, viruses, fungi, and parasites, against their respective treatments.
2. Can my body become resistant to antibiotics?
No, this is a common misconception. Your body does not become immune or resistant to the drug. Instead, it is the bacteria living in or infecting your body that develop or acquire resistance to the medication.
3. Why are antibiotics completely useless against the common cold and flu?
The common cold, influenza (flu), and most seasonal sore throats are caused by viruses. Antibiotics are biochemically designed to target the cellular structures and metabolic pathways of bacteria only. They have absolutely no effect on viruses. Taking them for a viral infection only destroys your body’s healthy gut bacteria and promotes the selection of antibiotic-resistant bacteria.
4. What happens if I stop taking my prescribed antibiotic course early because I feel better?
When you stop taking your medication early, you may have killed off the weakest bacteria, making you feel better temporarily. However, the most resilient and mutated bacteria survive. By cutting the course short, you leave these dangerous survivors alive to multiply and mutate, potentially causing a relapse that the same antibiotic will no longer be able to cure.
5. How can an ordinary citizen help stop the silent pandemic of AMR?
You can take immediate action by following three golden rules: Never demand antibiotics from a doctor or pharmacist, never self-medicate or share leftover antibiotics with family members, and always complete the exact course prescribed by a certified medical professional, even if you feel completely recovered mid-way.